


A silent threat. Prostate cancer is the most common cancer in men in England, yet early stages rarely cause symptoms. PSA screening reduces prostate cancer mortality by 20%.
A single baseline test predicts decades of risk. A PSA test at age 45-50 is one of the most useful predictors of future prostate cancer risk. Levels below 1.0 ng/ml suggest very low risk over the following decade; levels above 1.0 warrant closer monitoring.
MRI first, biopsy later. When PSA is elevated, an MRI is now the standard first step. It can rule out significant cancer with 90% accuracy, sparing many men an invasive biopsy.
A diagnosis is not a treatment order. Low-risk prostate cancer is typically managed with active surveillance - regular monitoring rather than immediate surgery or radiotherapy - without compromising survival.
Introduction
Over 50,000 men in the UK will be diagnosed with prostate cancer this year. More than 11,000 will die from it - one man every 45 minutes. Prostate cancer is now the most common cancer in England, surpassing breast cancer in women by number of diagnoses. These are not abstract figures: they represent men who felt well, had no symptoms, and had no reason to think anything was wrong.
That last point matters. Prostate cancer is a silent disease. By the time symptoms appear - difficulty urinating, unexplained back pain - cancer has often already spread beyond the prostate. Screening exists precisely because waiting for symptoms is waiting too long.
When researchers followed 180,000 European men for 16 years, they found that PSA screening reduces prostate cancer mortality by 20% and cuts the risk of metastatic cancer - cancer that has spread to other organs - by nearly a third.
A PSA blood test, ordered at a routine GP appointment, can change that outcome.
What PSA Actually Measures
PSA - prostate specific antigen - is a protein produced by the prostate gland. When the prostate is healthy, PSA levels in the blood stay low. When it is inflamed (prostatitis), enlarged (benign prostatic hyperplasia), or cancerous, PSA levels can rise. The test is a signal, not a diagnosis: it tells you something needs investigating, not what that something is.
For years, this ambiguity was the test's central weakness. The development of MRI-guided follow-up, described below, is what changed the picture.
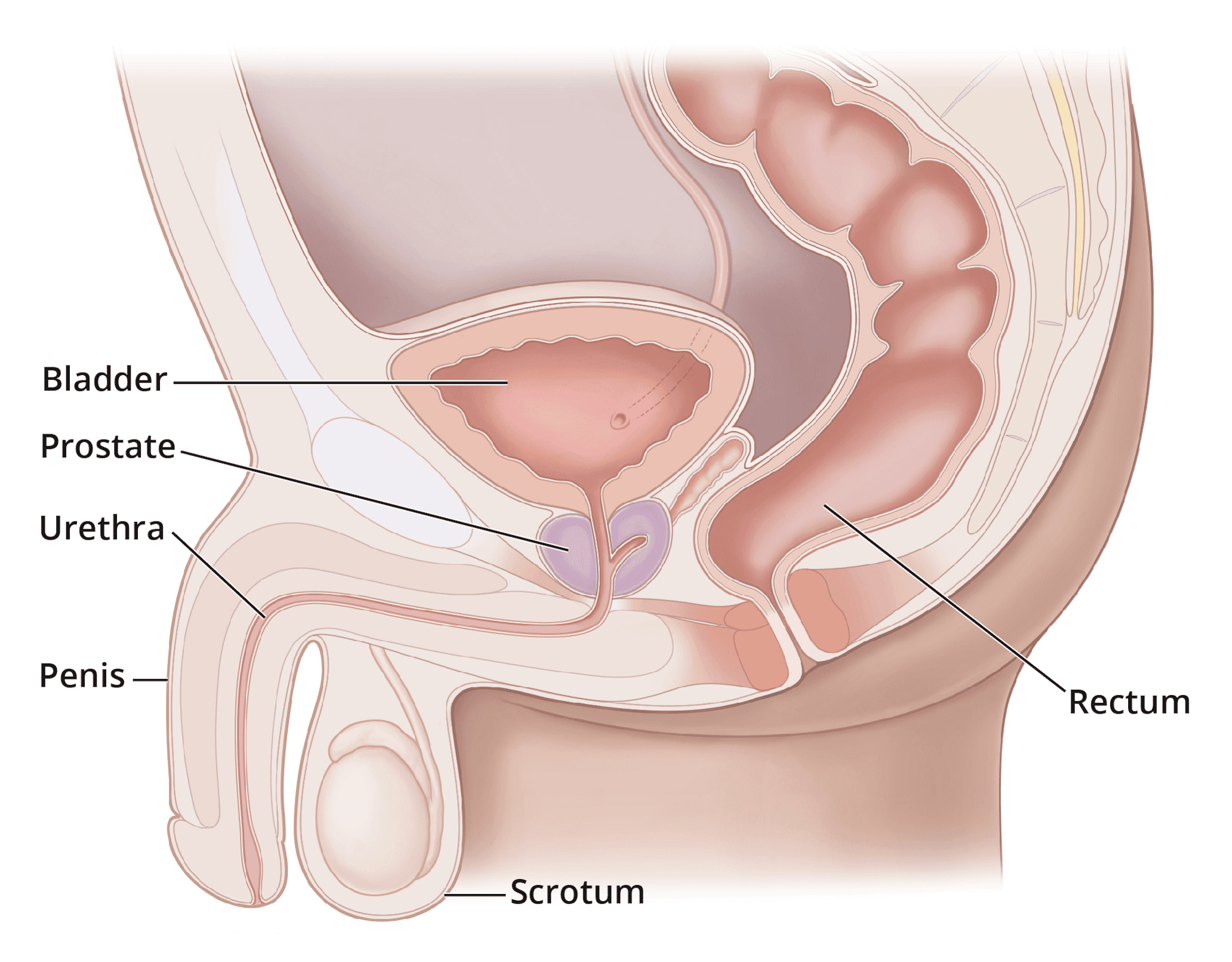
Figure 1 - Diagram of the Prostate
Discover the 5 habits that boost your longevity
Unlock a doctor-reviewed 5-day guide to the core pillars of long-term health—diet, exercise, lifestyle, sleep, and mental wellbeing. Evidence-based, practical, and designed to help you start making meaningful changes today.
No spam. Unsubscribe anytime.
By continuing, you agree to receive occasional updates from Emerald. See our Privacy Policy.
PSA and Age
PSA levels rise naturally with age, so the threshold for concern shifts depending on where you are in life.
In your 40s and 50s, the median PSA is 0.6 to 0.7 ng/ml. Anything above 1.0 warrants more frequent monitoring; anything above 2.5 ng/ml should prompt a referral to a urologist.
In your 60s, the threshold rises to 4.0 ng/ml, with typical levels between 1.0 and 1.5 ng/ml.
Over 70, levels naturally climb higher and interpretation becomes more individual.
But one number carries particular weight: your PSA at age 45. Men with a PSA below 1.0 ng/ml at that age have a very low risk of aggressive cancer over the following decade and can safely test every three years. Men with a PSA above 1.0 ng/ml at that age should test annually. If PSA rises by more than 0.75 ng/ml per year, regardless of the absolute level, a doctor should be consulted.
Investigating an elevated PSA
An elevated PSA once meant an almost automatic biopsy - a needle procedure through the rectal wall, with a 1-2% risk of serious infection and a high rate of identifying cancers that would never have caused harm. That approach has been largely replaced.
Multiparametric MRI is now the recommended first step when PSA is raised or rising. It can rule out significant cancer with 90% accuracy. In clinical trials, adding MRI before biopsy halved the number of unnecessary cancer diagnoses - meaning fewer men labelled with a cancer that required no treatment, and fewer subjected to biopsies that produced no useful information.
When biopsy is still needed
If MRI identifies a suspicious area, biopsy remains necessary. The technique has improved substantially. MRI-ultrasound fusion technology overlays the MRI scan onto a real-time ultrasound image, allowing the doctor to direct the biopsy needle precisely rather than sampling at random. The 2024 evidence shows this targeted approach detects aggressive cancers while finding 50% fewer harmless ones.
The biopsy route has also changed. The standard approach now goes through the perineum - the skin between the scrotum and rectum - rather than through the rectal wall. This has effectively eliminated the infection risk associated with the older technique. The procedure is done as an outpatient, and general anaesthetic is available for those who want it, though post-procedure discomfort when urinating is common for a short period.
Longevity starts with awareness
Less than £1/day. Test 115+ biomarkers. Personalised plan and 1:1 GP support.
Who Needs Treatment?
Finding prostate cancer does not automatically mean treating it. This is one of the most important shifts in the field and still one of the least understood.
The ProtecT trial, led by Oxford University, followed men with prostate cancer for over a decade. For low-risk cancers, there was no difference in survival between men who had immediate surgery, immediate radiotherapy, or careful monitoring alone. Both NICE in the UK and the National Cancer Institute in the US have updated their guidelines accordingly.
Men diagnosed with low-grade prostate cancer are now typically offered active surveillance: regular PSA tests, periodic MRIs, and treatment only if the cancer shows signs of progression. This avoids surgery and radiotherapy - and their potential side effects of urinary incontinence and erectile dysfunction - while keeping the option of treatment available if needed.
Should I Get Screened?
Screening recommendations vary by individual risk, not just age.
Higher risk - consider screening from age 40-45 if you:
Are of Black African or Black Caribbean heritage: your risk of prostate cancer is approximately double that of white men.
Carry a BRCA2 gene mutation: this is associated with an eight-fold increase in prostate cancer risk.
Have a first-degree relative - father or brother - who had prostate cancer: your risk roughly doubles.
For men in these groups, annual PSA testing is a reasonable default.
Average risk - start at 50
For most men, the priority is a baseline PSA test between ages 45 and 50. That single result can shape your entire screening schedule going forward.
How old is too old to screen?
The question is less about age and more about life expectancy. An untreated early-stage prostate cancer typically takes ten years or more to become life-threatening. A healthy 75-year-old with no major comorbidities has good reason to keep screening. A 65-year-old with serious cardiovascular disease may not. This is a conversation worth having with your GP based on your individual picture.
A practical screening schedule
PSA under 1.0 ng/ml: retest in three years.
PSA 1.0-2.5 ng/ml: retest annually until stable, then every three years.
PSA above 2.5 ng/ml: referral to a urologist for further investigation.
If your PSA comes back elevated, repeat the test before acting on it. Several common factors can temporarily raise PSA: sexual activity within 48 hours of the test, vigorous exercise, urinary tract infections, prostatitis, and even constipation. If the elevated level persists on a second test, newer markers such as free PSA or the 4Kscore can help clarify whether further investigation is justified - evidence suggests they spare around 40% of men from unnecessary biopsy.
If a biopsy is recommended, ask about MRI-fusion guidance, the transperineal route, and how many samples are planned. Fewer, targeted samples generally mean fewer side effects.
Limitations of PSA
The debate around PSA screening is real and worth addressing honestly.
The US Preventive Services Task Force previously recommended against routine PSA screening, based largely on the PLCO trial, which appeared to show no mortality benefit. The problem is that the trial was poorly controlled: a substantial proportion of the 'unscreened' group had PSA tests during the study period, making any comparison unreliable. European trials using better-controlled methodology have consistently shown lives saved.
The concern about over-diagnosis - finding and treating cancers that would never have caused harm - was valid. But MRI-guided screening has largely resolved this at the diagnostic level, and active surveillance has resolved it at the treatment level. The version of PSA testing that warranted scepticism in 2010 no longer reflects current practice.
If your GP is reluctant to discuss PSA testing or digital rectal examination, or is working from guidelines that pre-date the MRI era, a referral to a urologist or a second opinion is reasonable.
The Future of PSA
PSA is increasingly used in combination with other markers rather than alone. The Swedish STHLM3 test combines PSA with genetic markers and clinical variables, achieving 74% accuracy in detecting clinically significant cancer compared to 56% for PSA alone. The 4Kscore panel provides a personalised risk estimate that helps decide whether biopsy is warranted. Both are available now, typically through specialist urology centres.
The broader picture is less encouraging. The Lancet Commission has projected that global prostate cancer cases will double by 2040, driven by ageing populations and rising incidence in low- and middle-income countries. The clinical tools now exist to manage this - PSA testing followed by MRI and targeted biopsy, applied through organised screening programmes rather than ad hoc testing. Whether health systems will implement them systematically is a separate question.
What This Means For You
PSA testing has moved from a blunt, contested screening tool to one component of a more precise system. The key changes are: MRI before biopsy, targeted biopsy when biopsy is needed, and active surveillance for low-risk disease. Each step reduces harm and increases the accuracy of what follows.
If you are over 45 and have not had a baseline PSA test, book a GP appointment and ask for one. If you have risk factors - Black heritage, a BRCA2 mutation, or a first-degree relative with prostate cancer - that conversation should happen earlier.
Early prostate cancer has no symptoms. That is the only fact you need to act on.
References
Hugosson J, Roobol MJ, Månsson M, et al. A 16-yr follow-up of the European Randomized Study of Screening for Prostate Cancer. European Urology. 2019;76(1):43-51.
Hugosson J, Månsson M, Wallström J, et al. Prostate Cancer Screening with PSA and MRI Followed by Targeted Biopsy Only. New England Journal of Medicine. 2022;387(23):2126-2137.
The Lancet Commission. The Lancet Commission on prostate cancer: planning for the surge in cases. The Lancet. 2024;403(10437):1683-1722.
Hamdy FC, Donovan JL, Lane JA, et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer (ProtecT Trial). New England Journal of Medicine. 2016;375:1415-1424.
Nordström T, Discacciati A, Bergman M, et al. Prostate cancer screening using a combination of risk-prediction, MRI, and targeted prostate biopsies (STHLM3-MRI): a prospective, population-based, randomised, open-label, non-inferiority trial. The Lancet Oncology. 2021;22(9):1240-1249.
Auvinen A, Tammela TLJ, Mirtti T, et al. Prostate Cancer Screening With PSA, Kallikrein Panel, and MRI: The ProScreen Randomized Trial. JAMA. 2024;331(17):1452-1459.
Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. The Lancet. 2017;389(10071):815-822.
Early Detection of Prostate Cancer: AUA/SUO Guideline. American Urological Association. 2023. Available at: https://www.auanet.org/guidelines-and-quality/guidelines/early-detection-of-prostate-cancer-guidelines
Mottet N, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer. European Urology. 2024;79(2):243-262.



Test 115+ biomarkers for fine-tuning your health
See your results in 3 days with high-level accuracy and a certified GP-reviewed action plan
