

A finite number: You are born with your lifetime egg supply. While quantity drops naturally, egg quality is the real driver of age-related decline and miscarriage risk—and unlike quantity, quality cannot be measured by a simple blood test.
Fertility goes beyond the ovaries: Fertility is orchestrated by the brain as well as the ovaries. If the body perceives high stress, low energy, or poor metabolic health, it may suppress ovulation to prioritise survival over reproduction.
Some diseases can impact fertility: Conditions like PCOS, endometriosis, or silent tubal issues can impact fertility early on, and male factor issues contribute to 50% of all conception struggles.
Optimising the odds: Biology is responsive. Lifestyle choices—specifically metabolic health and nutrition—support the system’s current function, while egg freezing and IVF are modern tools to help navigate or extend biological timelines.
Introduction
Fertility has become one of the most emotionally charged words in modern health discourse. It appears in headlines about declining birth rates. It surfaces in conversations about career timing. It’s debated in policy, romanticised in wellness culture, and medicalised in clinic corridors. Somewhere between the statistics and the social pressure, something important gets lost: Fertility is a biological system.
And like any complex system, it functions best when understood. At Emerald, we believe that clarity dismantles fear. So, this is not a countdown clock narrative. It is not alarmism. It is not reassurance for reassurance’s sake. This is a detailed, evidence-based, biologically grounded guide to how female fertility works, why it changes, why some women struggle even in their 20s, how lifestyle shapes reproductive physiology, and how modern technology has expanded what is possible. Consider this your blueprint.
Discover the 5 habits that boost your longevity
Unlock a doctor-reviewed 5-day guide to the core pillars of long-term health—diet, exercise, lifestyle, sleep, and mental wellbeing. Evidence-based, practical, and designed to help you start making meaningful changes today.
No spam. Unsubscribe anytime.
By continuing, you agree to receive occasional updates from Emerald. See our Privacy Policy.
Understanding the Biology
Before you are born
To understand fertility, we begin before birth. Unlike men, who produce sperm continuously from puberty onward, women are born with their lifetime supply of eggs (oocytes). During foetal development, around week 20 of the pregnancy, the ovaries in an unborn foetus contain approximately 6–7 million oocytes. By birth, this number has already fallen to 1–2 million. By the time a girl reaches puberty, around 300,000 remain. Across an entire adult life, only around 300–500 eggs will ever be released in a process known as ovulation.
This finite egg reserve is the first key principle of female fertility. There is no replenishment or regeneration. The ovarian reserve is established before you are born.
How eggs are released
Each month women of reproductive age (usually 15-49) release an egg in a process known as ovulation. For this to happen the ovaries recruit a small group of follicles. Under the influence of hormones (FSH), one follicle becomes 'dominant'. That follicle releases an egg at ovulation. The remaining follicles naturally break down and are reabsorbed by the body.
How egg quality changes over time
As the years pass and eggs are released monthly during the menstrual cycle, two distinct processes occur:
A decline in egg quantity (ovarian reserve)
A decline in egg quality (genetic integrity)
These processes are related but not identical. Inside each egg is delicate cellular machinery responsible for dividing chromosomes evenly during fertilisation. This process, known as meiosis, requires precise alignment and separation of genetic material to ensure chromosomes are correctly divided and ready to combine with the sperm’s genetic material. As we age, the structures responsible for dividing genetic material become less reliable. This means chromosomes may not separate properly, increasing the chance of eggs having the wrong number of chromosomes. This can lead to complications when trying to have a baby.
Embryos with damages genetic information often:
Fail to implant
Result in early miscarriage
Develop chromosomal conditions
This is why miscarriage rates increase with maternal age and why fertility declines are primarily driven by egg quality rather than simply egg number. Importantly, there is no blood test that directly measures egg quality. Age remains the strongest predictor.
How the brain and ovaries interact
Fertility is not located in the ovaries alone. It is orchestrated by the brain. The hypothalamus (a gland in the brain) releases regular timed bursts of a hormone called GnRH. The pituitary (also in the brain) responds by secreting two more hormones FSH and LH. The ovaries respond by producing oestrogen and progesterone. This is the hypothalamic–pituitary–ovarian (HPO) axis and it works like a series of commands given out by the boss and carried out by the workers (in this example, the ovaries).
The rhythm of GnRH release determines whether ovulation occurs. If that signal changes, ovulation may be delayed or suppressed. Now that we understand this it becomes clearer why the system is highly sensitive to what’s happening in your body and environment — including how much energy you’re taking in, how stressed you are, your thyroid function, hormone levels, body composition, and even how well you’re sleeping.
In evolutionary terms, reproduction requires safety. If the brain perceives famine, instability, or physiological threat, it will suppress reproductive signalling. This is why fertility is not just reproductive health. It is metabolic health, neurological health and psychological health.
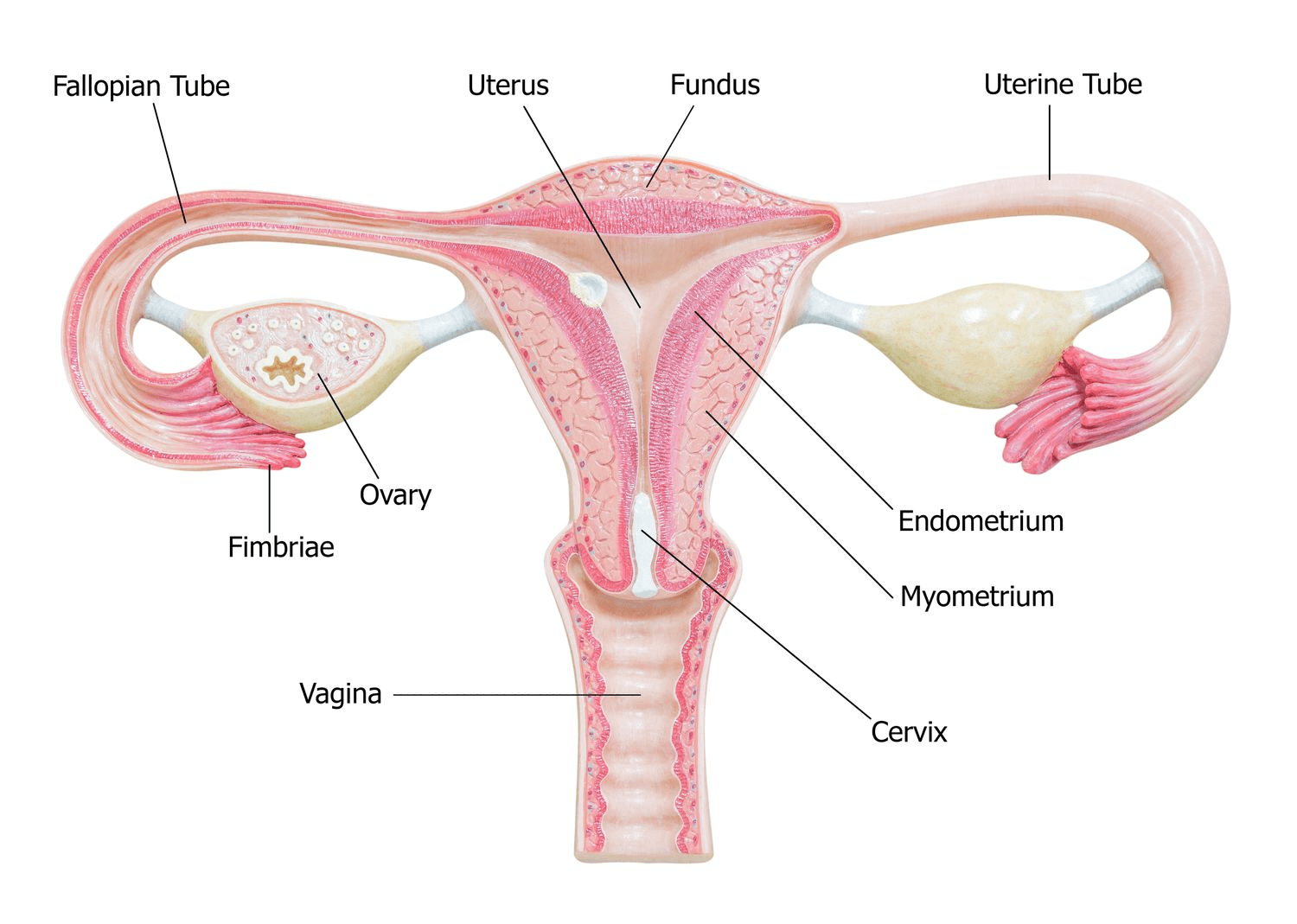
The Uterus
The uterus is not passive. Each cycle, under the influence of oestrogen, the lining of the endometrium thickens. After ovulation, progesterone stabilises and transforms this lining into a receptive state. There is a narrow “window of implantation”. This is typically around days 6–10 after ovulation during which the endometrium is biochemically primed to accept an embryo. Successful implantation requires synchronisation between embryo development and endometrial receptivity. Even minor timing disruptions can affect implantation rates.
The immune system plays a crucial role in fertility. The body is designed to react to anything foreign, but a developing embryo is partly different from the mother, making it a unique exception. To support implantation the uterus must tolerate the embryo while still maintaining the ability to defend itself against infections. Specialised immune cells, including natural killer cells and regulatory T cells, help maintain this balance by promoting tolerance and controlling inflammation. Cytokines and other signalling molecules carefully orchestrate this environment creating a window where the embryo can implant safely. This intricate interplay is essential for successful conception and early pregnancy.
Why some women struggle to conceive
The assumption that fertility is effortless in youth is one of the most harmful myths in reproductive health. While fertility statistically peaks in the 20s, many women in this decade have trouble conceiving. These challenges reflect biological variation and underlying medical factors rather than any personal failing.
Ovulatory Disorders
Polycystic Ovary Syndrome (PCOS) affects up to 10% of women. It is characterised by:
Irregular or absent ovulation
Elevated androgens
Insulin resistance
In PCOS, follicles begin to develop but fail to mature and ovulate regularly. Without ovulation, conception cannot occur. Hypothalamic amenorrhoea is another cause of anovulation. It often affects high-performing, highly active women who are under significant stress or in sustained calorie deficit. The brain reduces GnRH pulsatility, suppressing ovulation entirely. Thyroid disorders and elevated prolactin can also interfere with ovulation.
Endometriosis
Endometriosis affects approximately 10% of reproductive-age women. Endometriosis is not just “painful periods.” It is a long-term condition where tissue similar to the lining of the womb starts to grow outside of it — often around the ovaries, fallopian tubes, or other structures in the pelvis.
Over time, this can affect fertility in several ways. The inflammation caused by this tissue can lead to scar tissue forming, which may change the normal position of the ovaries and fallopian tubes, making it harder for the egg and sperm to meet. The environment within the pelvis can also become less favourable for conception. Inflammation can interfere with how the egg, sperm, and embryo interact, and in more severe cases, it may affect egg quality or how well an embryo implants. Importantly, the impact on fertility is not always obvious. Some women with severe symptoms conceive without difficulty, while others with milder symptoms may experience challenges.
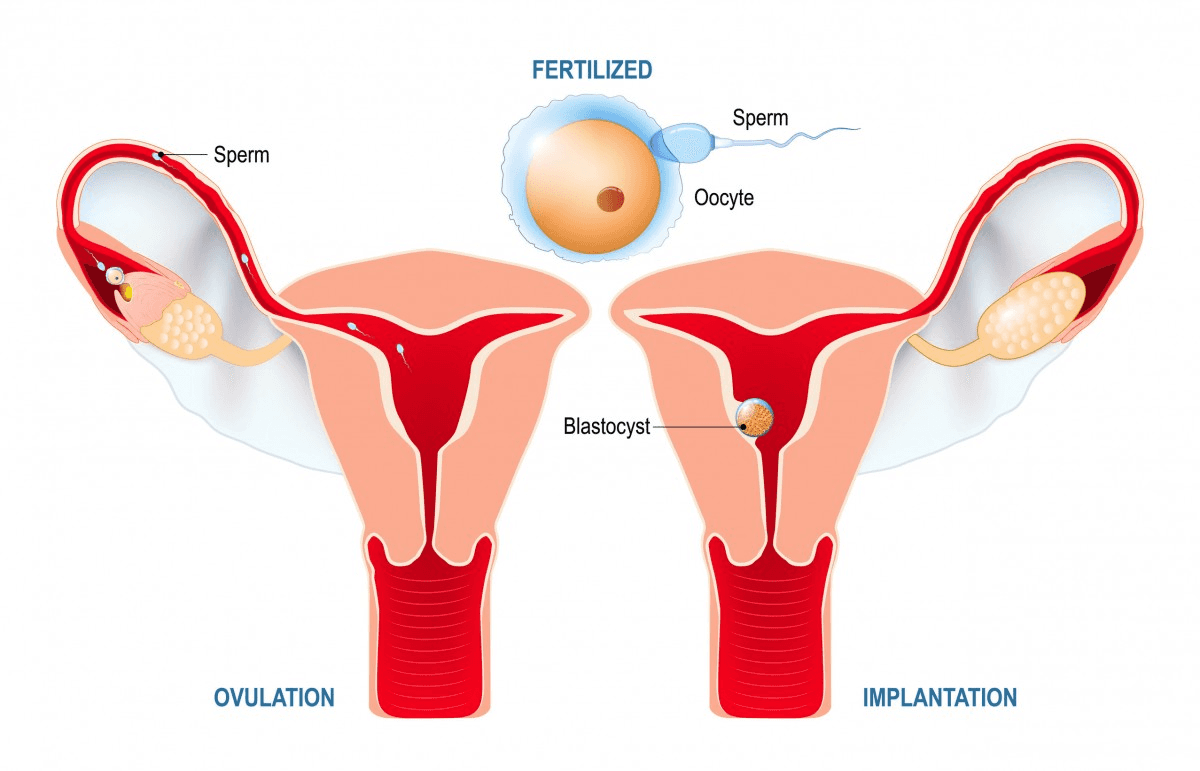
Tubal Factor
Fertilisation occurs within the fallopian tube. Damage to this structure, either from previous infections, inflammation, surgery or ectopic pregnancy, can prevent sperm and egg from meeting. Problems with the fallopian tubes often don’t cause any symptoms and are only picked up when someone is being investigated for fertility.
Diminished Ovarian Reserve
In some women, the number of eggs in the ovaries can decline earlier than expected. This can be influenced by things like genetics, certain medical conditions, previous ovarian surgery, or treatments such as chemotherapy or radiotherapy. In some cases, no clear cause is found. This early decline — sometimes called premature ovarian insufficiency — can happen in the 20s or early 30s.
Male Factors
Up to 50% of infertility cases involve sperm parameters. It is of course important to acknowledge that fertility reflects both male and female physiology.
Longevity starts with awareness
Less than £1/day. Test 115+ biomarkers. Personalised plan and 1:1 GP support.
Lifestyle and fertility
While fertility cannot be fully controlled, it is biologically responsive. Body Composition and Metabolic Health Both underweight states and obesity can disrupt ovulation. Excess visceral fat increases inflammatory cytokines and insulin resistance. Elevated insulin can increase ovarian androgen production, disrupting follicular development. Conversely, severe caloric restriction suppresses GnRH variability. The body favours stability.
Nutrition
A Mediterranean-style dietary pattern has been associated with improved fertility outcomes. This pattern emphasises:
Fibre-rich vegetables and legumes
Omega-3 fatty acids
Healthy fats such as olive oil
Adequate iron intake
Zinc and selenium
Vitamin D sufficiency
Folic acid supplementation pre-conception
This diet supplies a wealth of antioxidants, essential fatty acids and micronutrients that support ovarian function. Antioxidants help neutralise oxidative stress which can damage eggs and impair follicle development. Omega 3 fatty acids reduce inflammation, support hormone balance and improve endometrial receptivity, enhancing the change of implantation. Additionally, the diet’s emphasis on high fibre stabilises blood sugar and insulin levels supporting ovulatory regularity, particularly in PCOS.
Exercise
Moderate resistance and cardiovascular exercise improve insulin sensitivity and metabolic function. Excessive endurance training combined with low energy availability can suppress ovulation. The system rewards balance over extremes.
Alcohol and Smoking
Smoking accelerates ovarian ageing and increases miscarriage risk. Heavy alcohol intake disrupts ovulation and oestrogen metabolism.
Stress
Chronic stress elevates cortisol. In some women, sustained cortisol elevation can interfere with ovulatory signalling. Psychological safety is physiologically relevant.
Fertility treatments
For some women, decisions around fertility preservation are shaped not by age, but by life circumstances. Treatments such as chemotherapy or pelvic radiotherapy can affect the ovaries and reduce the number of eggs. In these situations, options like egg or embryo freezing can help keep future possibilities open. Certain medical conditions or previous ovarian surgery may also lead to an earlier decline in egg numbers. Speaking to a fertility specialist early can help explore and preserve these options Modern reproductive medicine has transformed the landscape of possibility.
Egg Freezing
What to Expect
Stimulating the ovaries – You’ll take hormone injections for about 10–12 days to help your ovaries produce multiple eggs.
Monitoring progress – Doctors will check your ovaries with ultrasounds and blood tests to see how the eggs are developing.
Egg retrieval – The eggs are collected through a short procedure while you’re sedated, so you won’t feel pain.
Freezing the eggs – The eggs are quickly frozen using a method called vitrification to preserve their quality.
Key points:
Younger eggs generally have a better chance of success later on.
Freezing eggs preserves their quality, but it doesn’t guarantee a future pregnancy.
Possible side effects include mild bloating or discomfort, and rarely a more serious condition called ovarian hyperstimulation syndrome (OHSS).
IVF (In Vitro Fertilisation)
Eggs are retrieved, fertilised in a laboratory and cultured into embryos before transfer into the uterus.
IVF success is strongly tied to age. In women under 35, live birth rates per fresh IVF cycle are commonly around 40–50%, but this declines progressively with age to under 20% per cycle by age 40–42. Importantly, when multiple cycles (fresh + frozen embryo transfers) are considered, cumulative live birth rates can exceed 60% in younger women. Miscarriage rates after assisted conception also rise with age, reflecting changes in egg quality rather than the treatment itself. Modern strategies, such as single frozen embryo transfers and personalised stimulation protocols, have improved both safety and outcomes in IVF.
IVF Success Rates by Age (Approximate UK/Europe Figures)
Age Group | Live Birth Rate per Fresh IVF Cycle |
< 35 | ~40–50% |
35–37 | ~30–40% |
38–39 | ~20–30% |
40–42 | ~10–20% |
> 42 | < 10% |
These figures are broadly consistent with data from national registries (e.g., HFEA in the UK, ESHRE in Europe) and reflect average outcomes across clinics, recognising variation between individual programmes and patient health profiles.
ICSI
Intracytoplasmic sperm injection involves injecting a single sperm directly into an egg, improving fertilisation rates in male factor infertility.
Preimplantation Genetic Testing (PGT)
Embryos can be screened for chromosomal abnormalities before transfer, increasing implantation rates in selected groups.
Emerging Science
Research is advancing rapidly. Artificial intelligence is being used to grade embryos. Studies are exploring mitochondrial optimisation within eggs. The reproductive microbiome is being investigated for its role in implantation. Ovarian tissue preservation offers hope for cancer patients. Technology cannot fully override biology, but it continues to extend possibility.



Test 115+ biomarkers for fine-tuning your health
See your results in 3 days with high-level accuracy and a certified GP-reviewed action plan
